a. The Diagnostic Significance of Uric Acid Elimination
Description
This section is from the book "Part 9. Technique Of Reduction Cures And Gout - On the Pathology and Therapy of Disorders of Metabolism and Nutrition", by Prof. Dr. Carl von Noorden. Also available from Amazon: Clinical Treatises On the Pathology and Therapy of Disorders of Metabolism and Nutrition, Part 9.
a. The Diagnostic Significance of Uric Acid Elimination
In all those diseases that can be confounded with arthritis urica the elimination of endogenous uric acid is not so low as in chronic gout. There is one exception to this rule, namely, very old age. Here the metabolism of the nuclear substance is apparently reduced, and hence old people eliminate from 20 to 25% less uric acid on a purin-free diet than vigorous adult individuals. This point must, of course, always be considered in each case of gout occurring in an old person. I may add that the latter react to the introduction of purin containing material in the same way and with the same increase of the uric acid elimination as younger persons. In many articular disorders, especially in acute articular rheumatism, very high values for the endogenous uric acid may even be found (v. Herwerden, Zeitschr. f. klin. Med., 65. 19. 1908).
In non-gouty articular lesions, especially in chronic articular rheumatism and in arthrosis deformans, the purin bodies of the food reappear in the urine almost as promptly as in a healthy individual. It is true, I have occasionally seen a retardation of the elimination by one day; but on the following days the expected excretion of uric acid took place. In one case in which it was necessary to decide whether a chronic and painful swelling of the knee joint was of gouty origin or not we found the following values:
Endogenous uric acid values on the 4th to the 6th day of the purin-free diet:
0.46 g
0.42 g
0.45 g
Average 0.45 g
On the next 2 days the patient received 400 g. of beef (weighed raw), and then again for 4 days a purin-free diet; theoretically the ingestion of 800 g. of meat should have caused an elimination of 0.72 of uric acid. There were found:
0.49
0.97
0.56
0.44
0.53
0.43
Total 3.42
The endogenous uric acid excretion during the 6 days of observation should have been 2.7 g. (6 times 0.45 g.) ; as a matter of fact 0.72 g. more were eliminated, that is, exactly the calculated sum. So exact a correspondence will, of course, rarely be discovered. As a rule the reclaimed quantities of uric acid fluctuate by 10 to 15% upwards or downwards from the calculated sum. The prompt elimination of uric acid decidedly militated against the diagnosis of gout. Later a dense fibrous pseudoankylosis of the joint developed. This never occurs in arthritis urica, and hence definitely indicated (in the same sense as the metabolic study that had been performed half a year before) that the case belonged to the group of chronic articular forms of rheumatism.
In nephrolithiasis uratica the elimination of uric acid, after the administration of purin containing food, follows the ordinary rule. I find that in this disease the patients develop very high values for endogenous uric acid. In three cases, for instance, I was unsuccessful in reducing the uric acid elimination below 0.65, 0.72, 1.02, notwithstanding the fact that the patients lived on a strict milk diet for a whole week. In a number of other cases I noticed a low uric acid production, but the values for the uric acid always remained near the upper boundary of the normal. This seems to demonstrate that in the pathogenesis of uratic renal concretions an unusually high formation of uric acid may play a rôle, added, of course, to unfavorable conditions of solubility in the urine (high salt percentage, excess of acid phosphates). This may be due to the fact that these individuals are afflicted with increased nucleolysis or that a relatively large portion of the destroyed nucleinic acid is transformed into uric acid and only a relatively small portion to urea. Only such cases, of course, were considered in which the fresh urine contained no uric acid of older origin in the sediment.
In gout the results of examinations of this kind yield altogether different results, at least in certain stages of the disease. During the acute attack, as already mentioned, there occurs a spontaneous and very considerable increase of the urinary uric acid. It seems logical to conclude that at this time uric acid is washed out of urate deposits in joints, tophi, etc. Studies in regard to the production of exogenous uric acid during this time have not been made with sufficient thoroughness, and this problem is difficult to solve because one cannot decide how much of the uric acid increase is due to liberation of uric acid from urate deposits and how much to exogenous factors.
During the intervals between typical gouty attacks there are no doubt long periods during which the endogenous and the exogenous uric acid production is altogether normal, or, at least, varies so slightly from the normal that the deviations cannot be recognized. On the other hand, anomalous conditions may occur that do not correspond with the facts commonly observed in chronic atypical gout. Investigations in regard to the elimination of exogenous uric acid are, therefore, of diagnostic value in these studies only if they give a positive result, that is, if a considerable retardation in the uric acid elimination can be determined.
This constitutes no particular disadvantage as far as the diagnosis is concerned because typical cases of gout interrupted by free intervals offer no particular diagnostic difficulties, and because there will usually be found a tophus here and there that facilitates the diagnosis. In one case a positive result from this test proved to be of great value. The patient was a man who had never suffered from a typical attack of gout but had a typical gouty heredity (grandfather, father, and older brother). The patient consulted me in Frankfort en route to Homburg (1906), where he had been sent on account of fleeting neuralgiaform pains. These pains had been interpreted as symptoms precursory to gout, and, as was shown later, correctly. A metabolic study revealed great retention of exogenous uric acid, only a third of the expected quantity being found in the urine. This pointed to the diagnosis gout. About two weeks later, during the course of his cure in Homburg, the patient suffered his first typical attack of podagra.
In atypical chronic gout in which the local manifestations run an exceedingly slow course and in which periods altogether free from any disturbances do not occur or are exceedingly short, a retention of exogenous uric acid is almost invariably present. The endogenous uric acid excretion also deviates from the normal in so far as the values for the latter are usually exceptionally low, and in so far as greater fluctuations in the daily elimination are observed than in a healthy subject. If now to the purin-free diet purin containing material is added for two days the urinary elimination of uric acid increases only very slowly; or a short attempt at active elimination occurs that soon, however, becomes abortive. Even if the patient is placed for a whole week upon a purin-free diet after the expiration of the two meat days, only about one-half of the calculated amount of uric acid may reappear in the urine. This phenomenon is so constant that in doubtful cases it must be credited with great diagnostic importance. Therapeutically, too, it is valuable in so far as it indicates whether or not the patient should be troubled with the bothersome, occasionally dangerous and weakening restriction of purin containing foods.
I will now quote a few examples:
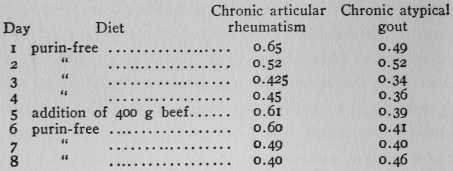
The 400 g. of beef should cause an elimination in the urine of 0.35 g. of uric acid over and above the endogenous value for uric acid. In the rheumatic individual this endogenous value (average of 3rd and 4th day) was 0.44 g. The increased elimination of the 5th and 6th day calculated together amounted to 0.33 g. The whole calculated quantity, therefore, appeared in the urine at the proper time.
In the gouty individual the endogenous uric acid value was 0.35 g. (average of the 4th and 5th days). The addition of meat produced a very much retarded increase in the uric acid elimination. Within 4 days only 0.26 g. instead of the expected 0.36 g. were eliminated (together 1.40 g., instead of 1.66 g.).
Continue to:
My Books

