b. The Therapeutic Significance of Tolerance Determinations
Description
This section is from the book "Part 9. Technique Of Reduction Cures And Gout - On the Pathology and Therapy of Disorders of Metabolism and Nutrition", by Prof. Dr. Carl von Noorden. Also available from Amazon: Clinical Treatises On the Pathology and Therapy of Disorders of Metabolism and Nutrition, Part 9.
b. The Therapeutic Significance of Tolerance Determinations
Three years and a half ago I called attention to the therapeutic importance of tolerance determinations in gouty subjects in a little monograph that I published together with my former assistant, L. Schliep (Berl. klin. Wochenschrift, 1905. No. 41). Even though we do not understand the exact nature of the gouty process, still all the facts that we are acquainted with to-day, as well as clinical experience, indicate that everything must be done in this disorder to prevent the retention of uric acid. One can take the stand that the best treatment is to exclude all purin containing material from the diet and this requirement would be filled by the use of vegetables, milk, and eggs (see below). Articles of this kind, provided they are given in sufficient quantity and in correct combinations supply a sufficient amount of adequately nourishing material. As a matter of fact, it is altogether rational in severe cases of the disease, especially in very painful forms of chronic arthritis urica to adopt this diet and to continue its use for weeks or even months at a time. The results obtained are frequently surprisingly good. I can remember a considerable number of cases in which the patients, while they did not get rid of the deformities that had occurred, nevertheless were spared all further difficulties, even though for years they had never been free from pain and had always been afflicted with new swellings. In some patients it is even necessary to maintain permanently a milk-egg-vegetable diet, because even the slightest addition of purin containing material to the food is not well tolerated and invariably precipitates new attacks.
Fortunately, however, only a small proportion of sufferers from gout is so completely intolerant to purin containing pabulum. In chronic atypical gout, as well as in the free intervals of typical gout there always remains a certain power of transforming and eliminating a limited quantity of purin material in a normal manner. The amount that can be utilized in this way corresponds to the boundary of tolerance. Danger does not accrue to these patients until this latter is exceeded, consequently it is important to know the boundary of tolerance. Conditions are here exactly similar as in diabetes mellitus. In the latter disease we have learned that it is forbidden and dangerous to adopt the routine of feeding every diabetic upon the same diet. We have learned to recognize that a most exact study of the tolerance of diabetics for carbohydrates must precede the regulation of the diet and that the latter must be adapted to individual peculiarities; for example, one patient will excrete sugar on 50 g. of bread, whereas another individual can tolerate 150 g. of bread without glycosuria; we find similar differences in the case of gouty subjects as far as their tolerance for purin containing material is concerned. Gout and diabetes, moreover, are related in this respect that the tolerance does not remain constant, but may fluctuate in either direction; such patients occasionally tolerating, more and at other times less purin containing material. An improvement in the tolerance may be attained therapeutically if the intake of purins is considerably reduced for a certain length of time, because in this way the uric acid forming function is, one may say, spared or rested, and an opportunity is given for its recuperation. It has also occasionally been observed that small quantities of purin containing material may in crease the excretion of uric acid more, relatively, than large quantities, and may even produce an absolutely higher uric acid excretion. Quite analogous conditions are found in diabetes.
An example of this kind is mentioned in the monograph quoted above (von Noorden and Schliep) ; another one is herewith submitted. The diet in this case had been purin-free for jive days preceding this investigation, but the urine was not analyzed:
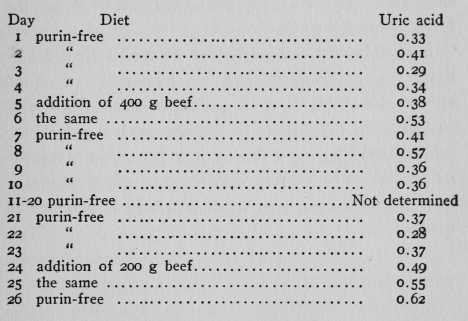
The endogenous uric acid excretion of this patient, who was afflicted with chronic atypical gout amounted to 0.34 g. (average of the 1st to 4th day). The addition of 800 g. of beef (400 g. on the 5th and 6th days) should have produced a plus of 0.72 of uric acid in the urine. As a matter of fact, from the 5th to the 8th day only an excess of 0.52 g. above the endogen ous value appeared, then the excretion became reduced. From the figures of the 21st to the 23rd day an endogenous average value of 0.34 g. could again be calculated. The addition of 400 g. of beef (200 g. for 2 days) should have produced 0.36 g. of uric acid, whereas the excess excretion of the 24th to the 26th day amounted to 0.64 g. The addition, therefore, of a smaller amount of beef not only relatively increased the uric acid elimination, but rendered it absolutely higher than the administration of the larger quantity of beef.
I need hardly call particular attention to the fact that (in contradistinction to commonly accepted views) the elimination of quantities of uric acid that are large in proportion to the amount of purin containing food ingested indicates a favorable condition of affairs. For a gouty individual is only then placed in a dangerous position when uric acid is retained in the body.
Continue to:
My Books

